What is pudendal neuralgia?
One of the rarer causes of chronic pelvic and genital pain is a disease called Pudendal Neuralgia. I have treated many patients over the past few years with this diagnosis.
The pudendal nerve is a very little known but very important nerve in the pelvis. It is a nerve that provides sensation to your inner buttocks, anus, perineum (the area between your anus and genitalia), and genitals. This nerve can be injured or irritated for many reasons. In roughly 50% of patients, we have no idea what triggered the issue. Some patients have Pudendal neuralgia from falling on their buttocks while snowboarding. It can be as simple as that. Some patients have endured serious surgeries such as pelvic sling mesh placement and have woken up with this pain. Regardless of the cause, the symptoms can be severely debilitating.
What are the symptoms?
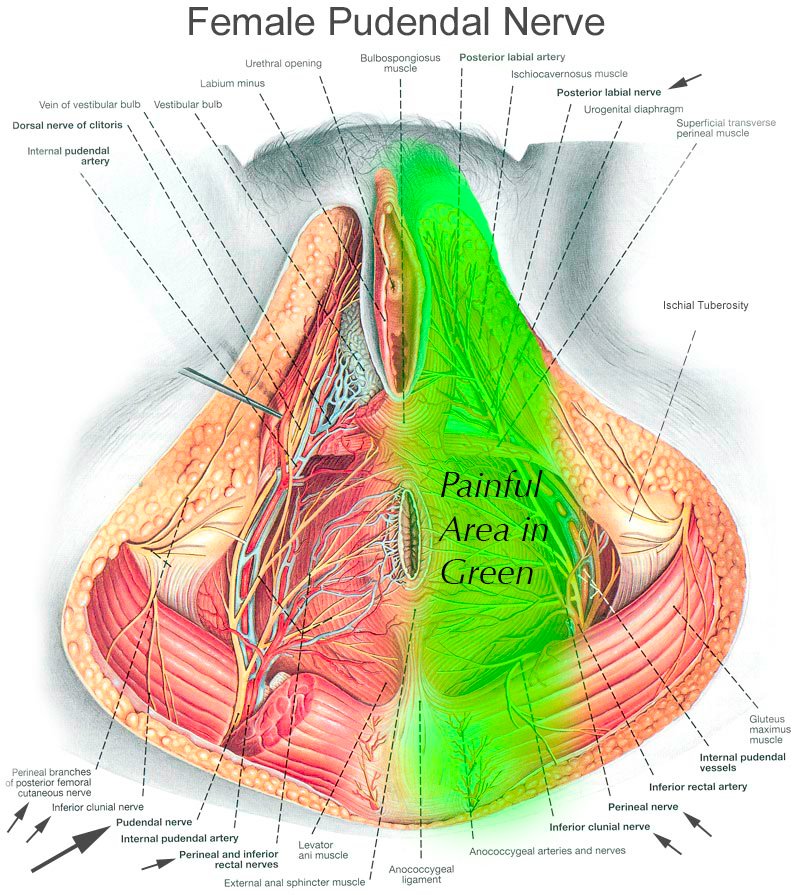
Typically my female patients with pudendal neuralgia experience severe perineal burning electrical pain and pain around the genitals, especially the vulva and the clitoris. They often complain of a sensation of “sitting on a rock” near their sitting bones (ischial tuberosities).
Men with pudendal neuralgia typically have pain more focused around the scrotum or end of the penis. The most common cause in men by far is extreme bicycling.
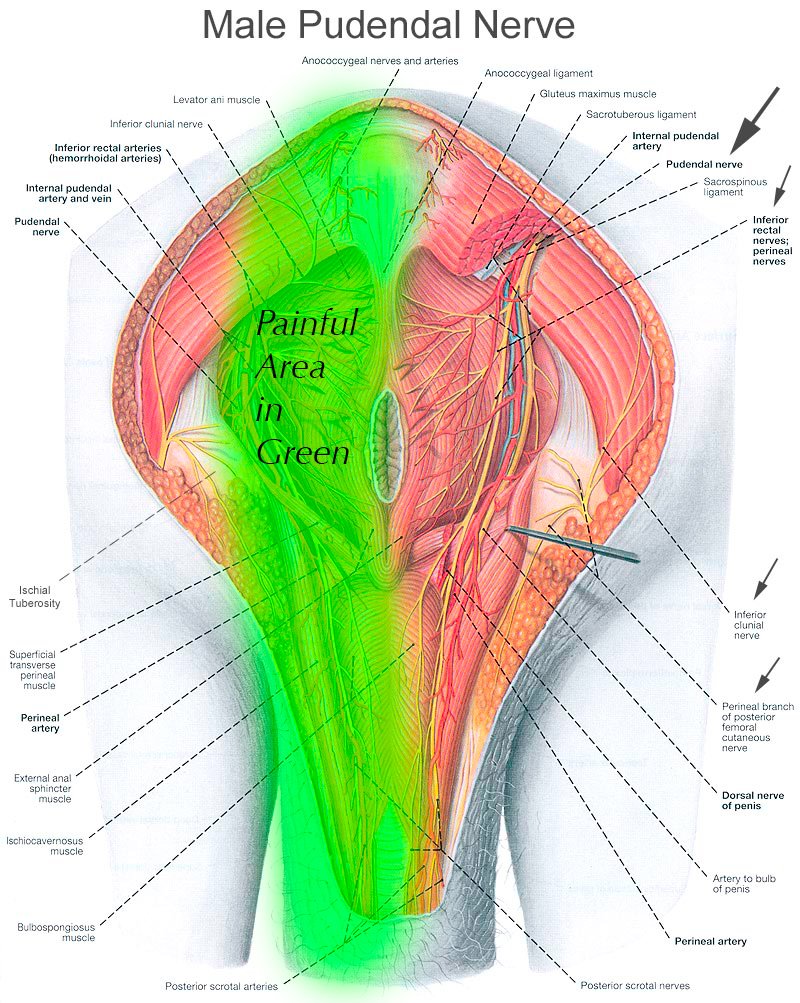
The images you see demonstrate the course of the pudendal nerve, and you can imagine that burning, electrical, stinging pain anywhere along this nerve would be extremely distressing.
How do pudendal neuralgia symptoms differ in women vs. in men?
In women, the pain is commonly in the perineum and vulva. In men, the pain is more common in the perineum and glans penis (tip of the penis).
What conditions can pudendal neuralgia be mistaken for?
Unfortunately, pudendal neuralgia symptoms are mirrored by many, many other diseases and syndromes. Almost always, other disease states need to be “ruled out” prior to pursuing a diagnosis of pudendal neuralgia. In women, endometriosis, vaginitis, UTI, vaginismus, or other infections need to be ruled out. In men, prostatitis and bladder issues need to be ruled out. I always encourage my female patients to be fully evaluated by a gynecologist or urogynecologist prior to seeing me if they have genital pain. They should also see a colorectal surgeon if there is severe rectal pain. My male patients should be evaluated by a urologist if they have genital pain. They should also see a colorectal surgeon if there is severe rectal pain.
I would estimate that 90% of the patients I see in my clinic who are later conclusively proven to have pudendal neuralgia have been misdiagnosed by multiple prior physicians. I have seen many women sterilized (had a historectomy) for this condition. I have seen many women have many invasive surgeries and long courses of antibiotics for this condition. Unfortunately this worsens the underlying problem.
Almost 100% of the men I see have been misdiagnosed with “prostatitis,” in the past, and had multiple courses of antibiotics.
What causes pudendal neuralgia?
In roughly 50% of cases, there is no known cause in women and men. In women, the most common known causes are pelvic floor surgeries by far, particularly pelvic mesh placement. In men, the most common known cause is trauma, in particular bicycling, falling on the buttocks during skiing or snowboarding, or violent masturbation.
To what extent can you prevent pudendal neuralgia?
Avoid extreme bicycling, avoid pelvic sling/mesh placement if possible.
What are the risk factors of pudendal neuralgia?
See causes, above.
Is pudental neuralgia hereditary?
Not to our knowledge. I have never had a patient mention pudendal neuralgia was present in any other family member.
Can pudendal neuralgia be treated?
Yes, there are many treatments!
Can it just go away by itself?
Yes, absolutely. However the longer you live with it, the less likely it is to go away by itself.
What are the treatment options?
The most conservative treatments include lifestyle modification, such as cessation of extreme bicycling. Other conservative options include pelvic floor physical therapy, in which a physical therapist places their fingers through the vagina and or rectum to stretch contracted pelvic floor muscles. Then medications can come into play, such has specially prepared vaginal or rectal suppositories with medications such as valium and baclofen which can help relax muscles and nerves in the pelvic floor. Oral medications such as muscle relaxants and nerve pain medications come next. Finally, invasive injection procedures enter the picture if needed. Such procedures include image-guided pudendal nerve blocks to diagnose the condition and hopefully gain some long term pain relief, image-guided pudendal nerve pulsed radiofrequency treatment, and image-guided botox injections of the obturator internus muscle to reduce pressure on the pudendal nerve as it passes through Alcock’s canal
There is a special combination procedure that I have invented for pudendal neuralgia . To my knowledge, I am the only physician in the world to offer this procedure. In this procedure, we inject nutrients around the pudendal nerve. These nutrients help to nourish the nerve and heal it. In addition, the fluid helps to release scar tissue from the nerve. This is called hydrodissection. I have found in most of my patients suffering from pudendal neuralgia also have hyperlax (loose) sacrotuberous ligaments. This ligament attaches the sacrum to the pelvis, and when damaged can irritate the pudendal nerve which travels directly underneath it. I therefore inject nutrienrts into the sacrotuberous ligament, which helps to strengthen it and prevent the ligament from releasing irritating inflammatory chemicals onto the nerve. In total, we can then nourish the nerve, free the nerve from scar tissue, and stabilize the surrounding ligaments.
We also perform cryoablation treatment to the pudendal nerve, in which a special machine is used to create an ice ball at the tip of a specialized needle. This ice ball literally freezes the pudendal nerve, and interrupts the pain signals on a long term basis. The nerve grows back unharmed after 6-12 months, but oftentimes the pain does not return with it. This is a neurodestructive treatment, and therefore not a treatment we utilize unless necessary.
Finally, the most invasive treatment I offer is called spinal cord stimulation, in which a special wire is placed along the spinal cord in the spine, and a small electrical current is applied to it. This blocks the pain signal from the pelvis to the brain. I use conventional spinal cord stimulator systems, as well as the newly released and very advanced St. Jude/Abbot DRG (dorsal root ganglion) stimulator, in which I can place these wires upon the S2-S4 nerve roots which form the pudendal nerve. This is a very powerful, expensive treatment, but one involving minor surgery, and thus I try save this option for last. You can read more about spinal cord stimulation in an interview I did with PudendalHope.
You can read about the St. Jude DRG stimulator here:
https://www.neuromodulation.abbott/us/en/chronic-pain.html
Oftentimes, particularly for patients traveling from foreign countries to see me, I will combine many of the procedures above in a single treatment. Therefore a patient may have pulsed radiofrequency treatement to the pudendal nerve, hydrodissection of the pudendal nerve, pulsed radiofrequency treatment of the pudendal nerve, botox to the obturator internus muscles, and nutrient rich injections to the sacrotuberous ligaments all in one session. The helps minimize the need to travel to my clinic multiple times to receive these treatments individually.
How does treatment work?
See above.
How long does pudendal neuralgia treatment take?
I treat nerve pain of all sorts all over the body. I want to be frank and state that pudendal neuralgia is one of the toughest to beat. Typically, treatment takes many months, when incorporating pelvic floor physical therapy, medications, injections, and lifestyle modifications. Patients typically will start with at least two diagnostic image-guided pudendal nerve blocks to confirm the diagnosis. They may then need to proceed to more advanced procedures such as pulsed radiofrequency treatement, botox, the PudendalRegen procedure, or in some cases spinal cord stimulation or dorsal root ganglion stimulation. Finally, surgical intervention may be needed in some cases.
Is there anyone who should not undergo treatment?
No, there is a treatment option of some sort for everybody.
What if I’m pregnant and have pudendal neuralgia?
If you are pregnant, you are only eligible for pelvic floor physical therapy and lifestyle modification. I do not offer injection or medication treatments for pregnant patients.
That said, I have never met a pregnant patient with chronic pudendal neuralgia. If they do have it, it is very transient.
How should I prepare for treatment so it goes smoothly?
We have specific instructions to help get the most out of your treatments, and these are provided to you as you enroll.
Can you walk me through what happens on treatment day?
For an injection, typically you will arrive at my clinic for check in. We will then discuss the procedure and answer all your questions and obtain written consent from you. We then perform various injecitons as described above, almost all of which involve using an ultrasound or x-ray machine to very precisely guide a very thin needle through the skin of your buttock to the pudendal nerve, obturator internus muscle, or sacrotuberous ligament. In general, I can do all procedures through a single needle poke, as I can redirect the needle deeper in your body to various targets. The injections last anywhere from 5 minutes to 45 minutes depending on which injection(s) you will receive. You are then sent home with a driver.
Do I need multiple visits?
Typically, yes, multiple injections are needed, but not always.
What aftercare do I need to do?
We have special protocols for you to follow depending on the treatment you are receiving.
What are signs of a smooth recovery?
Gradual reduction or elimination in your pain, however the pain typically fluctuates up and down for the first few weeks after treatment, so do not expect your pain to go away immediately.
How can I prevent pudendal neuralgia from returning?
See above.
How much does pudendal neuralgia treatment cost, and is it covered by insurance?
Treatment cost is often covered by insurance. Many procedure however are not covered by any insurance, and therefore need to be paid directly by you. Costs range from $300 to $3000 per side, depending on the complexity of the procedure performed.
How can I find a pudendal neuraglia doctor near me?
There are very few physicians that treat pudendal neuralgia in the entire world. This is truly unfortunate. I would suggest you visit pudendalhope.info for local physicians that may help you.
How do I know whether a given doctor can actually help me?
Ask them how many patients with pudendal neuralgia they have treated in their career. If it is less than 10, it is unlikely they have the expertise to help you. Unfortunely, 99.9% of physicians have never (knowingly) seen a single case of pudendal neuralgia.
If you are in pain and want to explore pudendal neuralgia treatment options, call Dr. Attaman’s Seattle office (206-395-4422) or Bellevue, WA office (425-247-3359), or email us to schedule an appointment.
